
New Nature Study Finds "No Correlation Between COVID-19 Vaccines And Fertility Issues"
And, as usual, that’s "normal" - because it’s utter junk and they haven’t really looked. A brief review.

Nature “pre-published”1 on January 21, 2026, a new study: “COVID-19 vaccination carries no association with childbirth rates in Sweden,” by Dennis Nordvall et al.2
As one of the earliest observers to document Sweden’s drop in birth rates starting in 2022, coinciding with the COVID-19 vaccine roll-out, and having continued to study fertility trends since, the topic immediately caught my attention.
To summarize the authors’ claim, COVID-19 vaccination is not causally associated with a reduction in childbirth among women of childbearing age. Based on Swedish registry data and a target-trial emulation-style analysis, the estimates are close to null.
Well, that should settle the debate.
However, as Dr Ah Kahn Syed pointed out when he first brought this study to my attention, things get - as usual with papers on COVID-19 vaccines in pregnancy - very dirty as soon as we get a little into the weeds of the paper.
Which claims are they confronting?
According to the authors, it’s “widely circulating speculative claims” which incited them to look at the issue.
Which claims specifically? No idea - as usual, they don’t feel it’s necessary to provide references to support this kind of statement.
I’m aware of substantiated claims - namely, that COVID vaccines roughly double the baseline miscarriage rate (see Arkmedic’s reanalysis of Shimabukuro et al.,3 and Guetzkow et al.’s analysis of Israeli insurer data4). I’m also cognizant of grotesque claims circulating around this issue, notably Yeadon and Latypova’s poison pills,5 6 whose assertions lack credible evidentiary support.
So it would be helpful to know which claims, precisely, the authors believe they are refuting in this paper. If it’s the idea that COVID vaccines would cause an 82% miscarriage rate and a 300% increase in stillbirths, as claimed by Latypova, we’re happy to concede - without resistance - that it can be safely regarded as a claim that collapses under the weight of its own absurdity.
If it’s the claim that authorizing COVID vaccines without an adequate safety basis or established benefit was a highly irresponsible decision - one that most likely resulted in a beyond-Thalidomide-level disaster - then settling that debate won’t be done by this study, as we’ll establish below.
Cohort Inconsistencies
As soon as we start reviewing how many pregnancies were studied, major inconsistencies appear. According to the abstract, the study concerns “a representative population of 369,000.” However, in the Methods section, the cohort is defined as “all women aged 18-45 who were residing in Jönköping County on January 1, 2021” (N = 59,773).
Throughout the rest of the paper and in the supplementary materials, 59,773 is the only cohort size that is clearly defined and used.
So where does the “369,000” figure in the abstract - the number most readers will retain - come from? It appears consistent with the approximate total population of Jönköping County (e.g., 368,856 residents as of December 31, 2023).7 If that is what the abstract is referring to, then it is at best confusing and at worst misleading, because it is not the population actually analyzed.
It took eleven authors to write and review this manuscript, yet the abstract still presents a cohort size that conflicts with the Methods. That does not inspire confidence in the care taken with other key details - especially for a paper making strong causal claims about vaccination and fertility.
Vaccinated versus Unvaccinated… Well, not really
In fact - and this is one of the study’s most problematic flaws - “vaccinated,” in the authors’ operational definition, means having received at least two doses, with follow-up censored at the third dose.
In other words, people who received only one dose are treated as “unvaccinated.” In a context where it is at least plausible (even if insufficiently studied) that a woman who experiences an adverse outcome - such as a miscarriage - after a first dose might be less likely to return for a second, this definition could introduce selection effects.
This is similar in spirit (though slightly less extreme) to the once-common practice of treating people as “unvaccinated” until 14 days after their second dose - an approach that became controversial because it distorts comparisons by misclassifying time at risk.
We can’t quantify the magnitude of any resulting bias from publicly available Swedish aggregate data, which lacks the necessary granularity.8
Nevertheless, this exposure definition is unacceptable as such, and should be handled explicitly and transparently, because it can (and will) materially affect interpretation.
At minimum, it changes the causal question from “vaccinated vs unvaccinated” to “completed the two-dose course vs a heterogeneous mixture of partially vaccinated and unvaccinated individuals.” Ideally, “dose-1 only” recipients should be analyzed separately, or the study should also report an “at least one dose” definition alongside the two-dose definition.
11 authors and not one who can code?
In a purported effort at transparency, the authors provided the R script used for their analysis.9 The code is severely deficient, enough to call into question the validity of the entire manuscript in its current form, even as a draft.
A few of the most egregious problems visible in a quick review:
1) An “exposure” definition that directly contradicts the study’s headline framing.
Exposure (i.e., the vaccination status used in the model) is defined - lines 48 to 51 - as having a recorded dose-2 date (“FörstaVaccinationDos2”). That confirms the design flaw discussed above: women who received only one dose are treated as “unvaccinated,” even though the paper is marketed as a clean “vaccinated versus unvaccinated” comparison.
2) Another major design flaw: events before dose 2 among eventual vaccinees are effectively dropped
The code tries to build a time-dependent Cox dataset by giving vaccinated women two rows:
Row A: unexposed from 2021-01-01 up to the dose-2 date
Row B: exposed from the dose-2 date to end of follow-up (or censoring)
That’s a standard start-stop approach in principle.
But what it actually does (around lines 77 and onward) is this:
For a vaccinated woman, the “last row” (sista) is the exposed row (the dose-2 row).
If she conceived before dose 2, then on that exposed row Kontaktdatum < Exposuredatum, so that row is removed by the Före==0 filter.
The remaining unexposed row still exists - but later the script forces all non-last rows to status <- 0.
Net result: conceptions that occur before dose 2 among women who later receive dose 2 are not counted as events anywhere. They’re not counted in the unexposed interval, and they’re not counted in the exposed interval. They simply vanish from the analysis.
That is textbook immortal time bias: eventual vaccinees are implicitly required to remain event-free until they receive dose 2, because events before dose 2 are discarded.
This will distort the hazard ratio - often toward “no association,” though the direction depends on how vaccination timing and conception timing are distributed. The crucial point is simpler: it breaks the risk-set logic of a time-dependent Cox model.
A correct implementation would keep the event in the interval where it actually occurs (almost always the unexposed interval) and stop follow-up at the event time.
3) The conception date calculation is internally inconsistent
The paper claims that conception is defined as 280 days prior to birth in the main analysis, with 266 days used only as a sensitivity analysis. The published code doesn’t match that. It effectively hardcodes 266 by overwriting the first assignment (lines 38-39):
Befruktningsdatum <- Kontaktdatum - 280
Befruktningsdatum <- Kontaktdatum - 266
That’s not a “sensitivity analysis.” It’s a bug.
And it’s not harmless: shifting conception dates by two weeks can move a non-trivial number of events across the “vaccinated vs unvaccinated” boundary when exposure is time-varying. That can wash out a signal and push estimates toward the null. The authors need to state plainly whether the reported estimates are affected by this.
4) Removing everyone with a miscarriage from the childbirth analysis
Line 128, on a “specific analysis on miscarriages”, the authors do:
comb <- comb[!(comb$Personnr %in% Missfall$Personnr),]
This exclusion of every woman who had a past history of miscarriage is not a benign cleanup, at all. It is conditioning, on a post-baseline event, that can be affected by vaccination, correlated with fertility, and correlated with healthcare-seeking and coding - none of which the authors properly examine.
If vaccination influences miscarriage risk even slightly, then excluding all women with miscarriages is a classic way to induce selection bias and to artificially attenuate an effect on births (because you’ve literally removed a pathway by which births can be reduced). In effect, it changes the estimand to something like “live birth among women who never have a recorded miscarriage,” which is not what the paper claims to estimate.
5) Miscarriage analysis contains a serious logic error: shifting dates instead of filtering
Around lines 335-337, the authors write:
#Remove miscarriages within 22 weeks after study start
n <- -154
FörstaMissfall21_ <- within(FörstaMissfall21_, Kontaktdatum <- as.Date(Kontaktdatum+n))
This does not remove miscarriages in the first 22 weeks after the study start. It subtracts 154 days from every miscarriage date - shifting all events earlier - and therefore changes event times and their classification relative to vaccination and censoring. That is almost certainly a bug.
If the intent was truly “exclude miscarriages occurring within 22 weeks after 2021-01-01,” the code should have filtered records, e.g.:
FörstaMissfall21_ <- FörstaMissfall21_[Kontaktdatum >= as.Date(”2021-01-01”) + 154, ]
To make matters worse, later the script merges with Missfall rather than FörstaMissfall21_, which looks like another object-name error.
6) Confounding control is minimal (and code reflects that)
The only adjusted covariate in the model is age at study start. That is not “causal modeling” in any serious sense, despite what the abstract implies. And even if the time-dependent handling were correct (it isn’t), a near-null estimate can easily reflect uncontrolled confounding - especially since vaccine uptake is socially patterned and plausibly correlated with pregnancy planning, healthcare contact, and other factors directly tied to childbirth outcomes.
Conclusion
I could go on with a long list of additional bugs, inconsistencies, and unused objects - but the point is clear: this code was never subjected to serious review, neither by the authors nor the reviewers.
As shown above, even if the obvious bugs were fixed, the analysis would still be at high risk of immortal-time bias, because it discards events occurring prior to dose 2 among eventual vaccinees. That alone is enough to say that a strong causal conclusion like “no causal association of vaccination with reduced childbirth” is not supported by the analysis as implemented.
Worse, the study doesn’t even provide a coherent exposure definition consistent with its headline framing, and the script is riddled with errors.
This was published in Nature in 2026, and it illustrates once again my mantra that peer review without full, audit-ready transparency is a dead model. This paper should be pulled offline to avoid misleading the public - and we can only wonder why none of the reviewers flagged these major issues.10
And when you see “Victoria Male” among the reviewers, that largely explains why no major issue was spotted.11
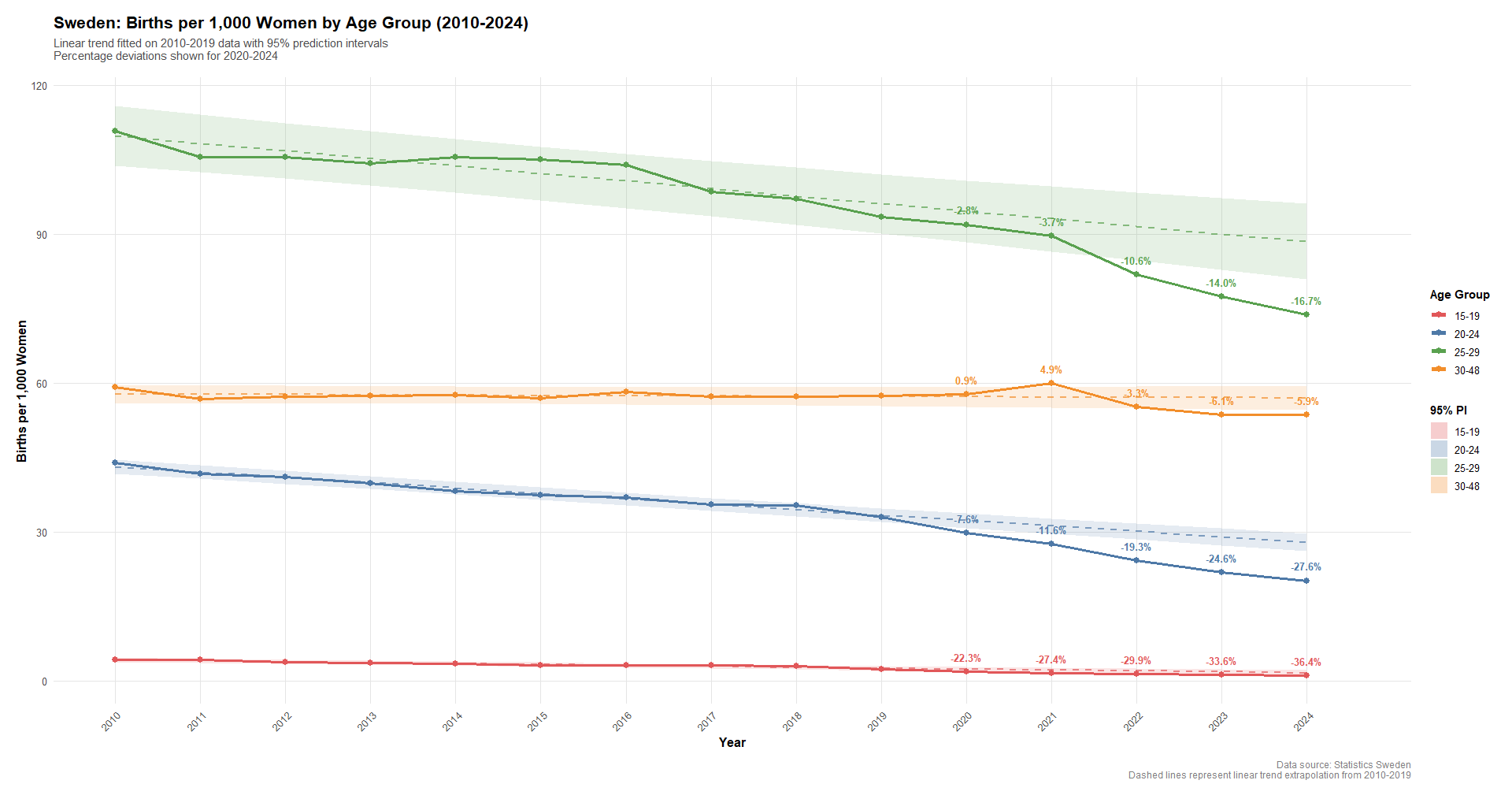
Meanwhile, births in Sweden,12 normalized by women in age,13 - among the ~82% recipients of at least one dose of COVID-19 vaccines in the 18-49 age groups range14 - look like this (R):
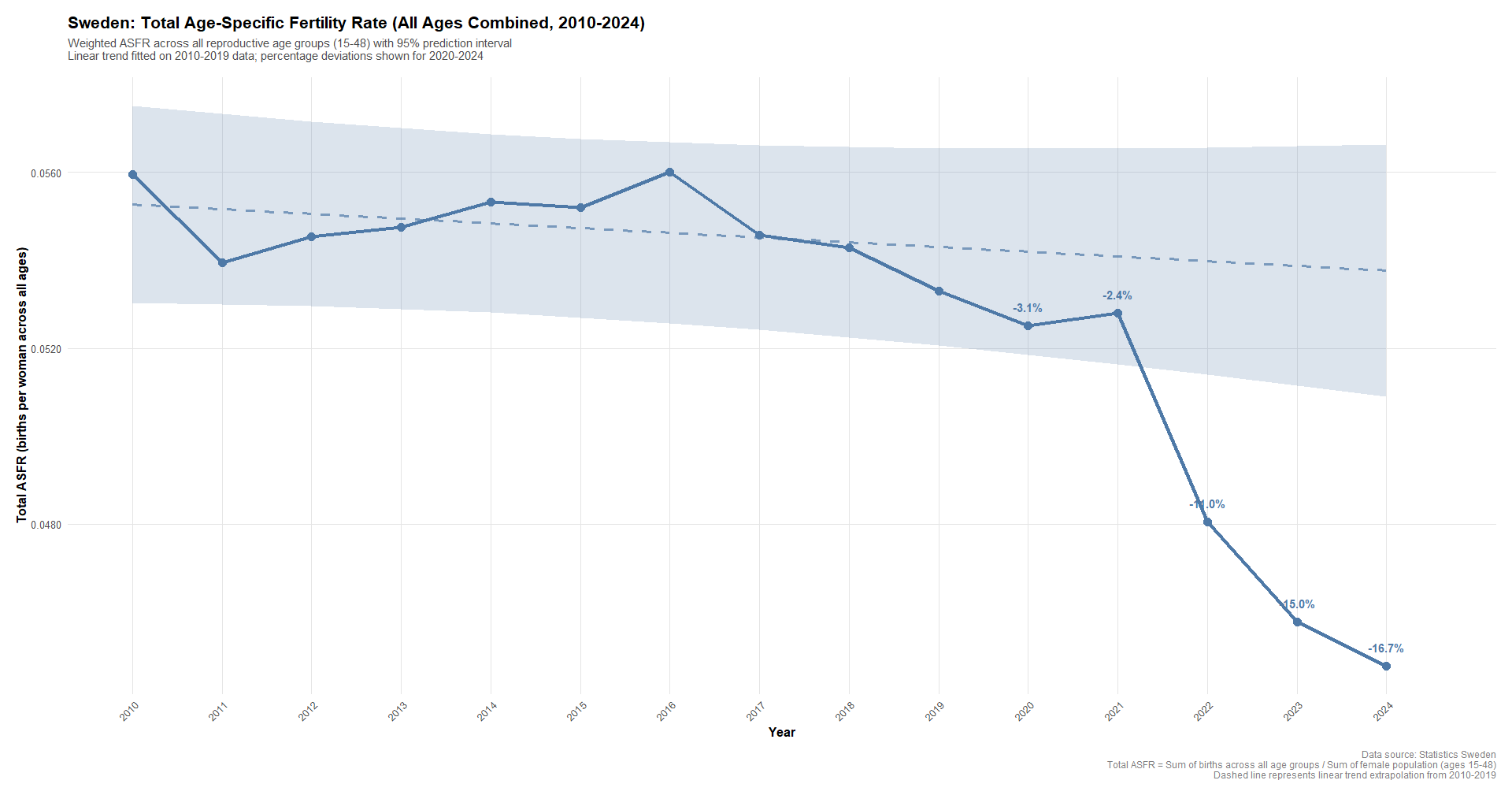
While the Age Standardized Fertility Rate (ASFR) looks like this:
Could we please have a decent, anonymized, individual-level dataset released for public audit, so this extremely serious question can be settled under conditions of basic competence and transparency - rather than behind closed doors, by biased reviewers and authors of questionable skill?
Meaning: “We can use our paper for propaganda purposes as if it were a real one, but once you’ve torn it apart, we won’t have to retract it - strictly speaking.”

https://zenodo.org/records/18138478 - Published January 3, 2026 | Version v1.0
https://blobserver.dc.scilifelab.se/blob/Folkhalsomyndigheten_Covid19_Vaccine-93.xlsx - From the sheet “Dos 1 till 3 per åldersgrupp” - By age band (Sweden): 18-29: 80.85% have received at least 1 dose, 30-39: 80.83% have received at least 1 dose, 40-49: 85.99% have received at least 1 dose.
For those who are not friendly to code.. this paper is a travesty of science, using a curated dataset that ends at a certain time whereas the paper itself claims a totally different end date. Essentially showing that the authors had no idea what they were doing and I would bet that this whole paper is ghost written for them.
They provide scripts (that they likely don't understand) but won't provide the data on which those scripts are supposed to be run, and have a "5 year" block on that data. Well I can tell you that any privacy concerns blocking that data release now will still exist in 5 years, so that is the most ridiculous thing I have seen in a paper.
:D
https://badprotein.substack.com/p/vger
https://badprotein.substack.com/p/vger
https://badprotein.substack.com/p/vger
https://badprotein.substack.com/p/vger
this shows why pfizer had to be FOIAed to get the distribution reports and mouse tissue damage.
they found things to stop the presses and their own studies told them so